Crosslinking with riboflavin and UV-A light has proven to be a first-line treatment for people with corneal ectasia disorders such as keratoconus, and pellucid marginal degeneration and corneal weakness (ectasia) after LASIK.
Photo-polymerisation with the use of ultra-violet light is the most promising technique to achieve cross-linking in connective tissue. Photo-polymerisation is activated by means of a non-toxic and soluble photomediator together with a wavelength of 365 nm UV-A light source.


Fig 2, shows UV-X in use for eye treatment.
Homogeneous UV-A irradiation of the corneal is an important factor for a safe treatment procedure.Thus a homogeneous illumination of the cornea with a patented beam and optics is essential - the IROC UV-X. UV-X was developed by an experience team of researchers in collaboration with the inventors of the procedure, Prof Theo Seiler and Prof Eberhard Spoerl. It is designed with a special focus on both safety and effectivity of the procedure, embodying the cutting-edge knowledge in the field of corneal cross-linking.

Fig 3, shows Scanning Electron microscopy image of the homogenizing micro-structure used in the UV-X.
Pictures of the UV-X treatment versus the LED techniques are shown below:

Fig 4, shows UV-A versus direct LED irradiation
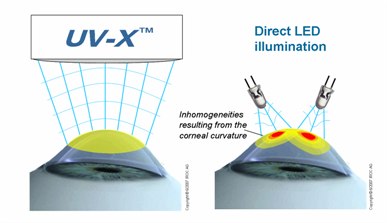
Fig 5, shows compensation of the corneal curvature using UV-X.

Fig 6, shows comparison of the treatment distance with reference to intensity-damage threshold.

Fig 7, shows an optical design according to Koehler's reduces the radiant exposure to retina.
Once patients have received crosslinking, in most cases their corneal shape will either remain stable or actually improve. This can provide patients with improved visual acuity and improved ability to wear contact lenses.
Some surgeons have also reported reasonable results in improving the stability of the cornea in people who have undergone radial keratotomy, an incisional refractive procedure from the 1980s and 1990s. Crosslinking appears to work best for those who are experiencing daily fluctuations in their vision.
Source: http://www.allaboutvision.com/conditions/corneal-crosslinking.htm

